Dynamic stabilisation
As an alternative to spinal fusion surgery, also known as spondylodesis, it is possible to reconstruct and stabilise the affected sections of the spine in a way that preserves movement, i.e. dynamically. When we consider the structure, function and requirements of the spine, it becomes clear what a complex organ it is. A healthy spine gives the human body mobility and stability without any pain. If structures in the spine are damaged as a result of degeneration, an accident or surgery, the balance between mobility and stability is disrupted. This malfunction typically leads to pain and is often the beginning of a whole cascade of secondary diseases of the spine. These can include:
- Degenerative scoliosis
- Degenerative instability
- Connection instability after previous stiffening
- spondylolisthesis
- Spondylarthrosis, facet joint arthrosis and spinal stenosis
- “Failed-back syndrome
- “Post-nucleotomy syndrome
The aim of spinal fusion surgery is to exclude the painful and diseased parts of the spine from the chain of movement. These spinal segments are fused and thus immobilised. Clinical studies have shown that spinal fusion surgery can often lead to painful secondary diseases in the adjacent segments. These, as well as the dreaded complication of implant loosening, may necessitate further surgical intervention. Based on these findings, the method of dynamic treatment has been developed.
Dynamic treatment of the diseased segments follows a completely different philosophy. It takes into account the fact that the spine cannot fulfil its function without the essential interplay of „stability and movement“. The aim of dynamic treatment surgery is to preserve the movement and function of the vertebral segments while eliminating the causes of pain. Various implants are available to the surgeon for this purpose.
Compared to other implants, the viscoelastic disc prosthesis has the advantage that its design perfectly mimics the function of the natural disc. Furthermore, extensive laboratory testing has proven that it has a durability of at least 50 years. Whether and how surgical treatment of the affected vertebral segments should be carried out is planned individually by the specialist after thorough diagnosis (MRI, CT, X-ray, physical and neurological examination). If, for certain reasons, partial fusion of a section of the spine is unavoidable, this should be limited to one segment as far as possible, as shown in the following example. In this way, the greatest possible functionality of the spine can be maintained or restored.
New clinical studies have shown that dynamic stabilisation of the spine is a sensible alternative to fusion surgery.

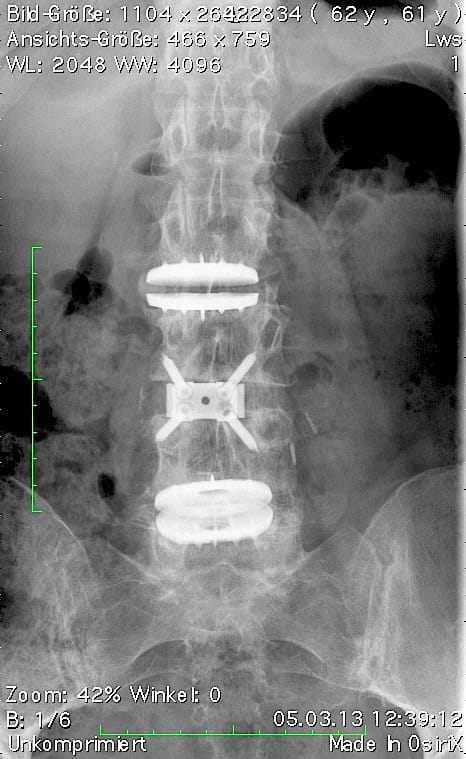

Postoperative status: Complete axial correction of the lumbar spine with two disc prostheses and a PEEK cage. Normal lordosis of the lumbar spine also visible in the lateral view after the operation. (Spine Centre Rischke)
(2) Example of treatment with a viscoelastic disc prosthesis and dynamic fixator in the presence of spondylolisthesis


References
Bertagnolli, R. (2011) Hybrid procedures, in: Bertagnolli, R. et al. Eds. Motion-preserving spinal surgery, Urban&Fischer, Munich
Rischke, B. (2013), in: Viscoelastic Lumbar Total Disc Replacement in the Treatment of Spondylolisthesis and Degenerative Scoliosis. http://www.isass.org/uploads/scoliosis/1.2.pptx/user/index.html?f=paper_scowro13.T-287Abscdgsbdc-Lumbar-Total-Disc-Replacement-in-the-Treatment-of-Spondylolisthesis-and-Degenerative-Scoliosis-Rischke.pdf
Park P. et al. (2013) Adjacent Segment Disease after Lumbar or Lumbosacral Fusion: Review of the Literature, Spine, Volume 29, Issue 17, Pages 1938–1944
Fribeck, P. et al. (2004) Adjacent Segment Disease after Lumbar or Lumbosacral Fusion: Review of the Literature, SPINE, Volume 29, Number 17, pp Page 1938-1944, Lippincott Williams & Wilkins Inc