Slipped disc
Prolapse and disc degeneration
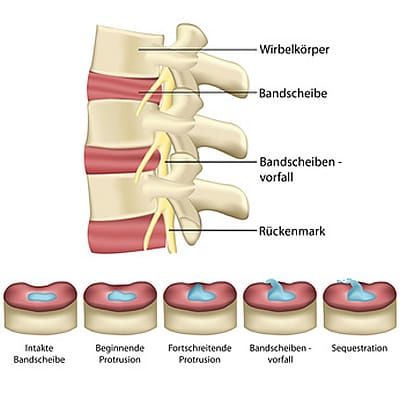
What is the structure of the intervertebral disc?
The intervertebral discs are firmly connected to the adjacent vertebrae and have the task of controlling the movement of the vertebrae and the load on the spine. The intervertebral disc consists of a fibrous ring (annulus fibrosus) made up of several intersecting collagen fibres. The overlapping fibrous rings create an elastic ring. The core of the intervertebral disc (nucleus pulposus) consists of a gelatinous, viscous protein tissue that is very firm and stable when healthy. This allows the load of the adjacent vertebrae to be transferred in a stable manner. However, the intervertebral disc does not contain any blood vessels (except in the embryonic stage). Nutrients are therefore supplied only by diffusion. Contrary to conventional wisdom and often-cited opinion, according to Alvin McKenzie (1) and Robert Roaf (2), it is not the intervertebral discs but the vertebral bodies that act as the actual shock absorbers. Under normal pressure loads below the critical load, a healthy intervertebral disc is displaced against the vertebral bodies, causing the elastic fibre ring to deform elastically. Under pressure, a healthy vertebra is able to stiffen itself through the very rapid inflow of fluid by tensing the muscles and thus bear the load (3).
What is a slipped disc?
A herniated disc is the result of degeneration and destruction of the disc ring and the gelatinous core. Chronic strain, a lack of tissue regeneration in old age, or injuries to the cartilage plates of the adjacent vertebral bodies lead to the destruction of the disc tissue. The lack of blood supply in the disc inevitably leads to a process of degeneration. Harmful inflammatory substances ultimately promote tissue degradation in a cascade-like manner. This leads to tears in the fibrous ring and, under pressure, to the escape of tissue fragments from the destroyed nucleus pulposus and/or the fibrous ring, which manifests itself as a disc prolapse or herniation. Since the fibrous ring is thinner in the rear section, the spinal canal and nerve roots can be compromised in this way (1). This results in pain, abnormal sensations or even paralysis in the arms or legs. In the case of a so-called mass prolapse, severe complications such as partial or complete paralysis of the spinal cord (paraplegia, cauda equina syndrome) can occur. (→see chapter: Therapy)
Treatment of herniated discs
Provided there are no nerve disorders in the form of abnormal sensations or nerve failure in the arms, hands, legs or feet, conservative treatment over several months is recommended. However, if there is no lasting improvement in symptoms and pain relief after this period, surgical treatment is usually unavoidable. Indications for surgery (4): – persistent nerve paralysis in the hands or feet – severe, untreatable pain and – acute bladder and/or rectal paralysis. In the lumbar spine, the spinal canal is usually opened from behind through a small incision of only a few centimetres with the aid of a microscope or endoscope. Compressive parts of a herniated disc can then be removed from the spinal canal, relieving pressure on the nerve roots. However, this type of therapy cannot reconstruct the degeneratively destroyed disc. The segmental collapse with its described pathologies remains. In the literature, the rate of recurrence due to a new disc herniation, instability-related damage to the spine, persistent painful symptoms and unsatisfactory results is estimated at up to 33%.[2,4,5,6] In these cases, the solution to this problem is to preserve movement and function by implanting a disc prosthesis. In the cervical spine, a herniated disc is usually operated on from the front, removing the entire disc tissue, thereby relieving the spinal canal and nerve roots. A spacer (cage) or disc prosthesis is then inserted to stabilise and reconstruct the spine.